Medically authored by Dr. Mario Quiros, MD — Board-Certified Emergency Medicine & Obesity Medicine Physician | Good Hearts Health
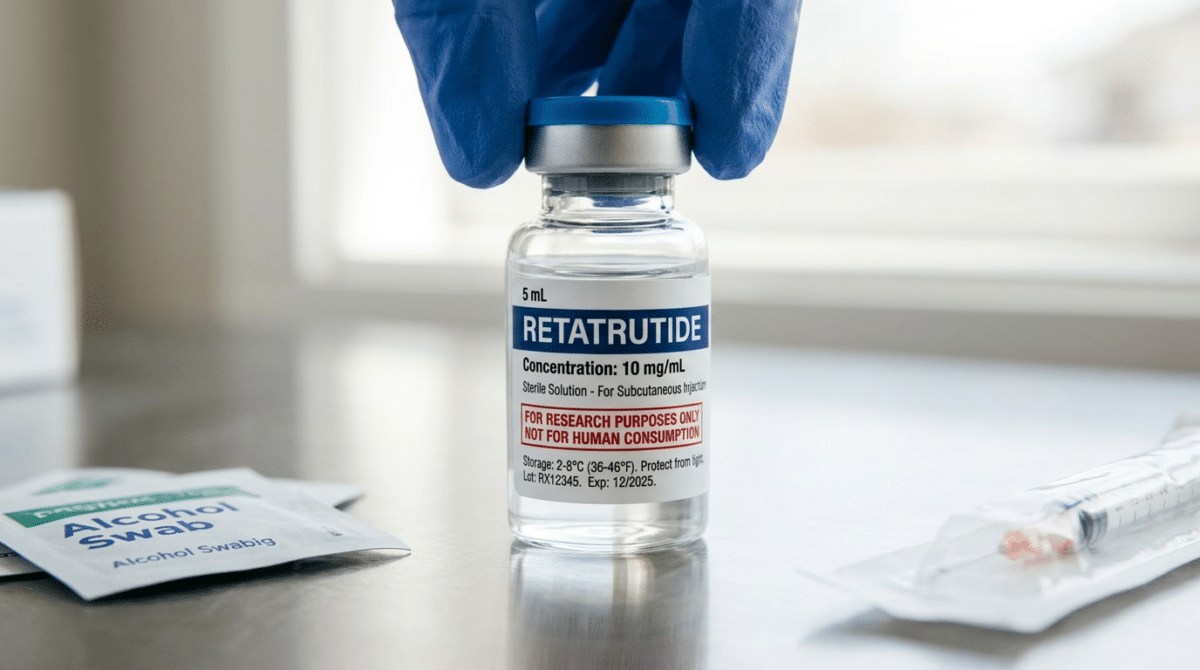
Retatrutide — nicknamed “triple G” or “GGG” in fitness communities — has become one of the most talked-about compounds in gym culture. Unlike semaglutide or tirzepatide, which carry FDA approval and physician oversight, retatrutide is not yet approved for human use. That hasn’t stopped it from flooding online peptide markets and underground supplement forums — and it hasn’t stopped men at gyms from injecting it.
As a physician who specializes in GLP-1 therapy and obesity medicine, what I’m seeing in this space concerns me deeply.
Why Retatrutide Has Exploded in Gym Culture
Retatrutide is a triple receptor agonist — it simultaneously activates the GLP-1, GIP, and glucagon receptors. Developed by Eli Lilly, the TRIUMPH-1 Phase 3 trial reported in May 2026 showed participants on the 12 mg dose lost an average of 70.3 lbs (28.3%) of body weight over 80 weeks — results unprecedented in the weight loss space.
What caught the attention of the bodybuilding and fitness community specifically was the glucagon component. Glucagon is a hormone associated with fat mobilization and energy expenditure, and the narrative that spread rapidly through fitness forums, YouTube channels, and private Discord groups became: “Retatrutide doesn’t just make you lose weight — it makes you lose fat while keeping your muscle.”
That narrative is, at best, misleading. At worst, it is dangerous.
The Stack: What Men in Gyms Are Combining with Retatrutide
The use of retatrutide in gym culture rarely happens in isolation. It is being used as part of what fitness communities call a “recomp stack” — compounds combined with the goal of simultaneously losing fat and preserving muscle. Common compounds being used alongside retatrutide include:
Anabolic Steroids
- Testosterone (various esters) — by far the most common co-administration. Testosterone directly stimulates muscle protein synthesis and counteracts the caloric deficit-driven muscle loss associated with GLP-1 therapy.
- Nandrolone (Deca-Durabolin) — favored for its joint-protective properties and muscle-preserving effects during aggressive cutting phases.
- Primobolan (Methenolone) — popular for lean muscle retention without significant water retention.
- Trenbolone — used by more advanced users for its potent fat-burning and muscle-hardening effects, though it carries significant cardiovascular and psychiatric risk.
SARMs (Selective Androgen Receptor Modulators)
- RAD-140 (Testolone) — marketed as a “safer” testosterone alternative for muscle preservation.
- LGD-4033 (Ligandrol) — used primarily for lean mass retention during caloric restriction.
- Ostarine (MK-2866) — widely promoted in fitness communities as muscle-sparing with minimal androgenic side effects.
Peptides and Growth Hormone Secretagogues
- Ipamorelin / CJC-1295 — growth hormone-releasing peptides used to boost HGH levels, muscle recovery, and fat metabolism.
- MK-677 (Ibutamoren) — an oral growth hormone secretagogue promoted for muscle gain and improved body composition.
- BPC-157 and TB-500 — promoted for recovery and tissue repair. As I have written about previously in my guide on peptide safety, both are FDA-banned for human use and lack long term safety and efficacy data.
Multi-GLP-1 Stacking
Some users are stacking retatrutide with tirzepatide or semaglutide in an attempt to create a more aggressive weight loss effect — a practice that carries significant risks including severe gastrointestinal complications, pancreatitis, and thyroid C-cell stimulation.
Why People Think Retatrutide Is Muscle-Sparing — And Why They’re Wrong
This is where the science matters most, and where gym culture’s anecdotal reporting is leading people astray. Phase 2 body composition data published in The Lancet Diabetes & Endocrinology showed that at the 12 mg dose over 48 weeks, approximately 74–75% of weight lost was fat mass, with 25–26% attributable to lean mass reduction. That lean mass figure is broadly comparable to other GLP-1 agents — there is no clinically validated evidence that retatrutide is uniquely muscle-sparing.
1. Confusing the Glucagon Effect with Muscle Protection
Yes, glucagon promotes fat oxidation. But glucagon is also catabolic — it can promote gluconeogenesis, the conversion of amino acids from muscle protein into glucose for energy. There is no reliable clinical evidence that retatrutide’s glucagon component selectively spares lean mass at the doses circulating in underground markets.
2. The Anabolics Are Doing the Work — Not Retatrutide
When someone stacks retatrutide with testosterone and reports “zero muscle loss,” the testosterone is almost certainly responsible for the muscle preservation. Exogenous testosterone dramatically increases muscle protein synthesis even in a significant caloric deficit. Attributing muscle-sparing to retatrutide in this context is a fundamental confounding variable error — and it spreads unchecked in communities where no physician oversight exists.
3. Short-Term Use Masks Long-Term Risk
Most users reporting favorable results are within the first 8 to 16 weeks of use. GLP-1-driven muscle loss tends to accelerate over time as the rate of weight loss outpaces the body’s ability to preserve lean tissue — particularly without adequate protein intake and structured resistance training.
4. Underground Market Doses Are Not Clinical Doses
The doses circulating in underground markets are often far higher or far lower than those studied in Phase 2 trials — with no quality assurance, sterility testing, or dosing accuracy. Exposures tracked by America’s Poison Centers surged to approximately 95 reports per month in early 2026, a 265% increase from the prior period.
5. Survivorship Bias in Online Reporting
The people posting physique updates and body recomposition success stories are, by definition, the ones who had positive experiences. The adverse events — significant muscle loss, cardiac arrhythmias, pancreatitis, severe nausea and malnutrition, severe hypoglycemia — do not get the same visibility on Instagram or fitness forums.
Why the Unregulated Status Is Fueling the Fire
Retatrutide is classified as a research chemical. It is not approved by the FDA for human use. It cannot be legally prescribed by a physician. The FDA issued warning letters to multiple websites in September 2025 for selling compounded or counterfeit retatrutide in violation of federal law. And yet it continues to be sold openly, often sourced from unregulated manufacturers — with no quality control on purity, potency, or sterility.
Several factors make the unregulated status a direct accelerant to its popularity in fitness culture:
- No prescription required. For gym communities already accustomed to purchasing SARMs and peptides through gray market channels, buying retatrutide online requires nothing more than a credit card and clicking a box stating it is “for research purposes only.”
- No physician oversight means no accountability. No one is monitoring cardiac function, thyroid markers, liver enzymes, or lean body mass. No one is adjusting the dose based on response. And critically, there is no one to call when something goes wrong.
- Significantly cheaper than FDA-approved GLP-1 therapy. Branded tirzepatide can cost several hundred dollars per month. Underground retatrutide is obtained at a fraction of that cost — with zero pharmaceutical-grade quality assurance.
- Exclusivity is reframed as desirability. In fitness culture, access to hard-to-obtain compounds carries social currency. The fact that retatrutide isn’t available at a pharmacy is reframed as a feature — “ahead of the curve,” “what the pros are using.” This makes the lack of FDA approval sound like an advantage rather than a serious safety signal.
- Regulatory lag on athletic prohibitions. While GLP-1 receptor agonists face increasing scrutiny in competitive sports, retatrutide’s specific inclusion on prohibited substance lists has not kept pace with its real-world use in athletic populations.
Dr. Q’s Take
Retatrutide may very well become a significant advance in obesity medicine once FDA review is complete. The Phase 3 trial data is genuinely promising. But the gym community’s adoption of an unapproved, unregulated compound — injected at self-determined doses, stacked with anabolic steroids and banned peptides — is not a preview of the future of weight loss medicine. It is an experiment being conducted on people who do not fully understand the risks they are taking.
The best results I see in my practice come from patients who are supervised, monitored, dosed appropriately, and supported throughout their weight loss journey. No online forum, peptide vendor, or fitness influencer can offer that.
Ready to Start a Safe, Physician-Supervised GLP-1 Weight Loss Program?
At Good Hearts Health, Dr. Mario Quiros provides personalized, board-certified concierge weight loss care using FDA-approved Semaglutide and Tirzepatide therapy. If you are considering GLP-1 therapy for weight loss, we offer a free initial consultation to see if our program is right for you.
Book your free consultation with Good Hearts Health today →
If you are experiencing any unexpected skin reactions, allergic responses, or side effects while using any GLP-1-class compound — whether FDA-approved or not — please consult a physician immediately.
References & Further Reading
- Eli Lilly TRIUMPH-1 Phase 3 Results: Retatrutide Delivered 28.3% Weight Loss Over 80 Weeks (May 2026)
- Eli Lilly TRIUMPH-4 Phase 3 Results: Retatrutide & Osteoarthritis (December 2025)
- Eli Lilly: What to Know About Retatrutide
- BioPharma Dive: Lilly’s Triple-Acting Obesity Drug Hits Goal in Phase 3 Trial
- The Lancet Diabetes & Endocrinology: Effects of Retatrutide on Body Composition — Phase 2 Substudy
- Cell Reports Medicine: GLP-1 Medicines Do Not Result in Disproportionate Muscle Mass Loss
- CBS News: This Weight-Loss Drug Hasn’t Been Approved by the FDA. Doctors Are Prescribing It Anyway.
- WUSF: People Are Buying Unregulated Injectable Peptides from Chinese Factories. Are They Safe?
- Drugs.com: What Is “Retatrutide Peptide” Being Sold Online?
- ClinicalTrials.gov: TRIUMPH Phase 3 Study of Retatrutide in Obesity/Overweight
Medically Authored by Dr. Mario Quiros, MD. Board-Certified Emergency Medicine and Obesity Medicine Physician. Owner and Operator of Good Hearts Health.